Progress in Mind
Choose a channel
Check out the different Progress in Mind content channels.
Correctly diagnosing Parkinson’s disease (PD) can be challenging, especially when based solely on medical history and physical examination techniques. While these form the basis of any diagnosis, Tao Xie, Chicago, USA, during a corporate-sponsored symposium at MDS 2018, explained how he uses DaT scan, in his everyday clinical practice.
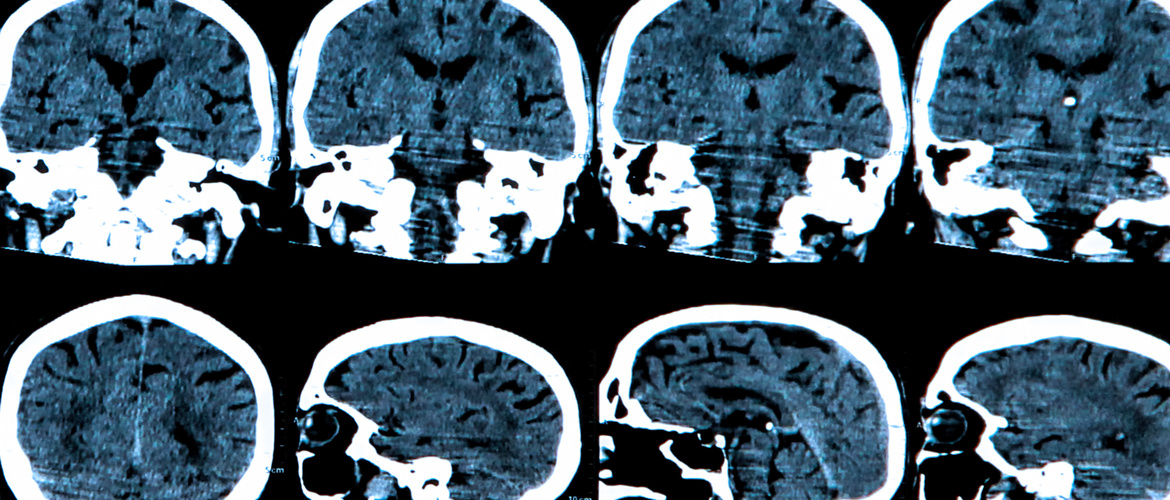
DaT scan is a single photon emission computer tomography (SPECT) nuclear imaging technique which uses a 123Iodine (123I)- labelled ligand bound to the dopamine transporter (DaT) to visualize functioning at the presynaptic dopaminergic neural terminal. A reduced DaT signal reflects presynaptic functional dopaminergic neuron loss.
In the EU, where it has been in use since 2000, DaT scan is clinically indicated in adults with clinically-uncertain Parkinsonian syndrome where its use can facilitate differentiation of essential tremor from tremor in Parkinsonian syndrome (PS) related to Parkinson’s disease (PD), multiple system atrophy (MSA) and progressive supranuclear palsy (PSP). It should be noted, however, that the technique does not distinguish between PD, MSA and PSP.
“Usually what you see in PD is asymmetric signal loss starting from the posterior putamen to the caudate nucleus. But be careful, abnormal imaging doesn’t equate with PD. It could be PSP, MSA or PD,” Dr Tao reported.
Abnormal imaging doesn’t equate with PD - it could be PSP, MSA or PD
The technique is also indicated in dementia where its use permits differentiation of probable dementia with Lewy bodies (DLB) from Alzheimer’s disease but it does not allow differentiation of DLB and PD dementia.
In the USA, where DaT scan has been in use since 2011, its indications are broader, allowing its use as an adjunct to other diagnostic evaluations in addition to differentiating ET from tremor due to PS related to PD, MSA and PSP.
Sensitivities and specificities of DaT scan use are as follows:
In clinically-uncertain Parkinsonian syndrome, 53% accuracy in early diagnosis without the scan versus 86-90% accuracy with the scan has been reported. [3]
In clinically-uncertain Parkinsonian syndrome, 53% accuracy in early diagnosis without the scan versus 86-90% accuracy with the scan has been reported
In general, Dr Tao reported, 50% or more of patients have their clinical management changed following DaT scan changed, depending on whether the technique is being used by a MDS specialist or not. Non-specialists tend to change clinical management strategies in a greater proportion of patients than specialists.
Essential tremor is not difficult to diagnose in most patients but can sometimes be challenging if it is present with symptoms mimicking Parkinsonism. And, he reminded the audience, patients with a long-standing essential tremor are also more likely to develop PD and, therefore, become ET/PD.
50% or more of patients have their clinical management changed following DaT scan changed
Cases demonstrate value of DaT scan in clinical practice
Dr Tao presented five case studies and among those, one case was exactly presenting essential tremor with symptoms mimicking Parkinsonism. Other cases illustrated the use of DaT scan in distinguishing psychogenic functional tremor from tremor-dominant PD, depression/catatonia from PD, Primary Lateral Sclerosis/Motor Neuron Disease from Multiple System Atrophy-Parkinson’s type and drug-induced PS from PD.
Dr Tao warned that certain medicines that bind to the dopamine transporter can interfere with diagnosis, including cannabis, and need to be discontinued prior to DaT scan.
Thus, this technique has been shown to help with early diagnosis in patients with uncertain tremor and Parkinsonism which in turn has led to their better earlier management with the avoidance of unnecessary testing, drug modifications, and unnecessary side-effects from use of inappropriate medicines.
This Symposium was conducted with educational financial support provided by GE Healthcare.